

Can A Strangulated Hernia Repair Itself
Affiliate 84
Abdominal Wall Reconstruction and Hernias
An abdominal hernia is any full-thickness defect or weakness in the wall of the belly that may permit protrusion of abdominal contents. Organ herniation through a ring of tissue bars within the abdominal crenel, such equally a diaphragmatic hernia or organ displacement through a mesenteric rent, is considered an internal abdominal hernia. This chapter discusses external wall defects only.
Definitions and Hernia Components
A hernia is composed of a ring (the anatomic limits of the wall defect), sometimes a sac, and the protruding contents (Figure 84-ane). The ring may be bars within a normal aperture in the abdominal wall (considered a truthful hernia) or may occur in other areas (fake hernias) every bit a result of trauma or through a disrupted surgical approach (an caused hernia). Very large hernial rings or minor defects rarely cause clinical problems; nonetheless, hernias just large enough to entrap viscera and obstruct blood supply to the contents (strangulation) are most dangerous to the patient. Contraction of scar tissue at the hernial band during the healing process may cause a delay in onset of clinical signs equally the organs become entrapped (incarcerated) or obstructed. Whereas in developmental (congenital) hernias, the hernial sac is a mesothelial membrane (peritoneum) roofing the contents, in acute traumatic or incisional hernias, no sac is present. Over time, a peritoneal sac may form over the contents of chronic traumatic or incisional hernias; this process is termed peritonealization. Hernial contents without a mesothelial covering are at take chances for developing adhesions that restrict motion of the contents (irreducible hernias); this may pb to obstruction or torsion of the protruding tissue. Traumatic hernias most often occur from blunt trauma with avulsion of muscle fascia or penetrating injury. When a traumatic abdominal hernia caused by a fractured rib penetrating through the paracostal musculature results in organ herniation, it is termed an auto-penetrating hernia.41,106 Contents of a hernia may exist predicted based on the site of the defect (e.g., inguinal hernias often have the uterus involved because of the tethering effect of the round ligament) or more mobile structures such as the omentum or intestine can travel longer distances into nearly any abdominal hernia site.
Anatomy of the Abdominal Wall
The tough intestinal wall confines the abdominal organs within the largest cavity in the body, extending from the diaphragm to the pelvic culvert (Figure 84-2). The arrangement of the aponeuroses of intestinal muscles, their attachments, and cobweb direction are important to understand when attempting hernia reconstruction. Fibers of the tendinous aponeuroses of the external abdominal oblique, internal abdominal oblique, and transverse intestinal muscles converge and join on midline to course a thick white band, termed the linea alba, which is located betwixt the rectus abdominis muscles. The linea alba is widest in the cranial abdomen, and it narrows considerably before information technology attaches to the pubis by the prepubic tendon (sometimes termed the cranial pubic ligament). Fibers of the flat tendinous aponeuroses of abdominal wall muscles pass either superficially or deep to the rectus abdominis muscles that extend in a cranial and caudal direction from the first costal cartilage to the pecten of the pubis. The external intestinal oblique aponeurosis ever runs superficial to the rectus abdominis muscle. The location of the aponeurosis of the internal abdominal oblique varies forth the length of the abdomen. In the cranial tertiary of the abdominal wall, fibers pass both deep and superficial to the rectus abdominis musculus. From the umbilicus caudally, all of the internal abdominal oblique fibers run superficial to the rectus abdominis muscle. Fibers of the transverse abdominal muscle pass deep to the rectus abdominis muscle in the cranial 2 thirds of the abdominal wall, only in the caudal third, fibers run superficial to the rectus abdominis muscle. Whereas the external rectus sheath contains tendinous aponeuroses of the abdominal muscles that run superficial to the rectus abdominis muscle, the internal rectus sheath is composed of sheets of fascia that are deep to this musculus. The external rectus sheath has been shown to be the primary strength-holding layer throughout ventral midline closures.101
On the lateral aspect of the abdomen, fibers of the external abdominal oblique muscles originate from the fourth or fifth to the twelfth rib and from the last rib and thoracodorsal fascia and extend in a caudoventral direction before giving rise to their wide aponeurosis. Fibers of the internal abdominal oblique musculus, which prevarication immediately deep to the external intestinal oblique musculus, arise from the thoracolumbar fascia caudal to the last rib and from the tuber coxae. These fibers extend cranioventrally, crossing the more superficial fibers of the external intestinal oblique muscles at about right angles. The deeper transverse abdominal muscle comes from two parts: the lumbar portion arises from the transverse processes of the lumbar vertebrae and the thoracolumbar fascia and the costal portion arises from the medial sides of the twelfth and thirteenth ribs and from the eighth to eleventh costal cartilages. Fibers from this muscle extend in a dorsoventral direction. The transverse fascia and peritoneum line the inner surface of this muscle. The beefcake of the inguinal and femoral triangle areas are discussed separately nether the inguinal and scrotal hernia and femoral hernia sections of this chapter.
Location of Abdominal Hernias
Although hernias tin can occur nearly anywhere in the abdominal wall, about defects are found in select areas (Figure 84-3). Cranial ventral midline hernias are nearly often congenital in origin and include umbilical hernias and substernal (or ventral) hernias. Defects in the more lateral areas of the abdominal wall most often result from trauma and include the paracostal defects only off the caudal rib margin or dorsal lateral hernias found just ventral to the lumbar transverse processes. Caudal abdominal hernias include congenital scrotal and inguinal hernias and those nearly often caused by trauma—the prepubic and femoral hernias.
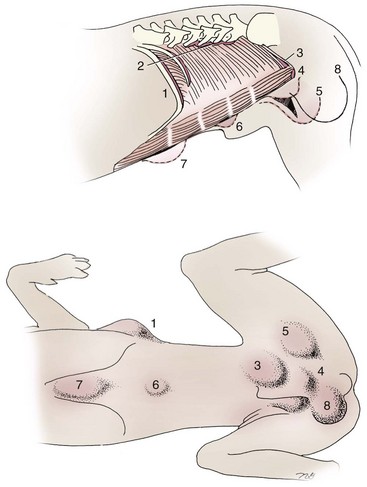
Effigy 84-3 Location of mutual abdominal hernias. Shaded areas indicate common regions of external swelling from the respective abdominal hernias. 1, Paracostal hernia; 2, dorsal lateral hernia; three, inguinal hernia; four, cranial pubic ligament rupture; 5, femoral hernia; half dozen, umbilical hernia; seven, ventral hernia (subxiphoid); and 8, scrotal hernia. (Modified from Smeak DD: Abdominal hernias. In Slatter DH, editor: Textbook of pocket-size animal surgery, ed 3, Philadelphia, 2003, Saunders/Elsevier.)
Incarceration
Incarceration of organs such equally the intestine, uterus, or float most often alters normal part because of luminal obstacle. Acutely incarcerated organs are irreducible and can become lethal strangulated obstructions within hours; therefore, urgent repair should be considered in this state of affairs. The severity and onset of the clinical signs related to the incarcerated obstacle oft depends on the contents of the hernia and size of the defect. Abdominal defects with pocket-size, inelastic hernial rings, such as scrotal or femoral hernias, are at high risk for incarceration and strangulation.120
Incarceration of the uterus may be associated with inguinal hernias or large umbilical hernias. An irreducible, feasible, nongravid uterus within a hernia rarely causes clinical bug; however, incarceration of a pyometra or gravid uterus may lead to severe systemic alterations and dystocia. Small intestine may become incarcerated inside any hernia; information technology is the writer's clinical impression that the risk is greatest when the hernial band approximates the size of the bowel. Larger hernias rarely trap or obstruct bowel unless they are acquired by acute trauma or the entrapped intestines undergo torsion. Intermittent intestinal dysfunction may occur, however, even if intestines are reducible inside the hernia. After signs of intestinal obstruction (acute abdominal pain, airsickness, depression, anorexia) occur, early intestinal decompression via exploratory laparotomy is warranted after patient stabilization. The urinary bladder may go obstructed in incarcerated perineal, ventral, inguinal, and traumatic pubic hernias. As urine menstruum becomes partially obstructed inside the hernia, the bladder progressively distends, further obstructing outflow. Immediate bladder decompression and diversion of urine flow can be provided via needle cystocentesis and catheterization; tube cystostomy is considered if the previous methods are unsuccessful. Surgical reduction of the float and hernia repair is attempted later the patient has been adequately stabilized.
Strangulation
A strangulated hernia implies that the hernial contents are incarcerated and undergoing devitalization from arrested apportionment. Arrested circulation may be from venous or arterial occlusion or a combination of the ii. Early venous obstruction results in reversible organ engorgement, merely somewhen arterial stagnation occurs from back pressure at the capillary beds. Arterial stagnation or obstruction causes rapid organ necrosis if the collateral claret supply is insufficient, resulting in organ rupture. Generally, venous obstruction occurs early in almost strangulated hernias, but by the time surgical decompression is attempted, irreversible arterial stagnation has occurred.
Strangulation occurs from several mechanisms, including constriction of the blood supply at the hernial band or torsion of the vascular pedicle with increased organ mobility. Organs with long, freely movable vascular pedicles (e.g., uterus, omentum, spleen, intestine, testicles) are more than prone to torsion. Incarceration of a hollow viscus favors strangulation considering increasing intraluminal pressure further obstructs venous outflow from the organ and opposes circulatory pressure. Traumatic hernias are at risk for delayed incarceration and strangulation because adhesions trap organs within the hernia, and contraction during wound healing eventually narrows the hernia ring.
The threat of complication and expiry is 50% college in humans with incarcerated or strangulated hernias than in hernias containing reducible viable tissue; therefore, early on diagnosis and surgical correction of incarcerated hernias is critical to prevent life-threatening sequelae relating to organ devitalization. Sequelae to hernia strangulation vary depending on chronicity and the organ involved. Strangulated umbilical, inguinal, femoral, and prepubic hernias nearly often contain falciform ligament or omentum, uterus, prostatic fat, and urinary float, respectively.108,120 The clinical grade of affected patients depends on the caste of vascular compromise, volume of body fluids lost from obstruction or sequestration, and absorption of bacteria and toxins. The presence of strangulated, contaminated hollow viscus may result in significant blood, protein, and fluid loss and frequently rupture, causing rapid toxemia and septicemia. Leaner drift transmurally through debilitated intestine even before evidence of gross spillage occurs.x Earlier overt signs of infection or contamination occur, vasoactive substances such as arachidonic acid metabolites, cytokines, leukotrienes, and kinins from tissue and blood cell autolysis crusade redistribution of trunk fluids and severe cardiopulmonary furnishings.xvi Strangulated viscera within external intestinal hernias may be more than isolated from the vascular system than those strangulated within the peritoneal cavity. Liberated vasoactive substances are not absorbed as apace through the subcutaneous tissue every bit the permeable intestinal crenel; thus, patients with external strangulated hernias may accept a more delayed onset of clinical signs and stupor. Severely compromised patients often decompensate and die under anesthesia during attempts at surgical reduction and repair of strangulated hernias; this is thought to be caused by rapid release of vasoactive substances into the circulation from necrotic strangulated organs during surgical reduction. En bloc resection of the devitalized herniated tissue, with release of the constricting ring only afterwards the vascular supply is occluded, may help reduce this fatal complexity.108
Principles of Abdominal Hernia Repair
The principal goals of hernia repair are to (ane) ensure the viability of entrapped hernia contents; (ii) release and return viable hernia contents into their normal location within abdominal cavity; (3) obliterate redundant hernia sac tissue; and (4) provide a tension-complimentary and secure primary closure of the defect using strong, good for you surrounding tissue. Acceptable surgical exposure and access to the hernia are important to assess hernia contents and isolate potent tissue for defect repair. If intestinal trauma is the suspected cause of a hernia, a midline celiotomy arroyo is preferred to allow the surgeon admission to the unabridged abdominal cavity to assess for concurrent injuries. Likewise, when strangulation of hernia contents is expected, a midline approach is recommended to isolate the abdominal cavity from the necrotic, often highly contaminated, local hernia environment. In uncomplicated hernias without evidence of obstacle or strangulation, an approach over the hernia rings is considered. Making an incision in a prophylactic region of the ring can facilitate release of the hernia contents. If the defect cannot be repaired primarily using direct approximation of local tissue, the pare and subcutaneous incision may be extended to provide admission for muscular or fascial flap evolution and defect reconstruction. Use of muscular or vascular fascial flaps is particularly important if the surgical site has gross contamination. When autogenous tissue cannot be used to close a large defect without undue tension, prosthetic implants may be considered, especially if the wound is considered clean. Polypropylene sheets are readily available and are often placed preperitoneally (within the intestinal wall) for a permanent abdominal wall substitute (see Reconstruction of Large Abdominal Hernias later in this chapter).
Surgical Conditions
Ventral Abdominal Hernias
Anatomy, Etiology, and Pathogenesis
In an embryo, the intestinal wall is formed by migration of cephalic, caudal, and lateral folds. The umbilical aperture, which serves as a passageway for the contents of the cord (umbilical blood vessels, small vitelline duct, and stalk of the allantois), remains after normal migration and fusion of these folds.62 The umbilicus is a cicatrix identifying the previous attachment site of the umbilical cord in a fetus. In mature animals, the falciform ligament (the remnant of the umbilical vein) and middle umbilical ligament of the float (the remnant of the urachus) are attached to the internal aspect of the umbilicus.35 Built umbilical hernias outcome from failure of fusion or delayed fusion of the lateral folds (principally, the rectus abdominis muscle and fascia) at the belly button afterward normal return of the midgut from the umbilical cord in the canine fetus, which ordinarily occurs at the sixth week of gestation.62 Most umbilical hernias are inherited and are probably the issue of a polygenic threshold graphic symbol, involving a major factor whose expression is mediated by the brood background.51,99 Until more is known near the inheritance and expression, affected dogs or cats should not be bred.
Umbilical hernias have been associated with fucosidosis, an inherited, autosomal recessive, neurovisceral lysosomal storage illness.115 Of 31 English language Springer spaniels with fucosidosis, 10 had umbilical hernias, and one had a scrotal hernia. This hernia has too been associated with a congenital, sex activity-linked, recessive disorder in dogs chosen ectodermal dysplasia.79
Cryptorchidism frequently coexists in dogs with umbilical hernias or other congenital defects.9,90 Congenital cranioventral abdominal hernias, incomplete caudal sternal fusion, and umbilical defects with concomitant diaphragmatic hernias of various types occur in dogs.81 Successive breedings of a Labrador retriever and an American foxhound with these defects created ratios of affected offspring suggestive of an autosomal recessive mechanism.36 Developmental causes were also suspected in a litter of cocker spaniels with diaphragmatic, cardiac, and abdominal wall defects similar to thoracoabdominal ectopic cordis syndrome.viii In humans, cardiac malposition may result in a mesodermal defect characterized past partial or complete failure of transverse septum development and supraumbilical fusion failure.25,28,62 Defects associated with infraumbilical midline hernias in humans include exstrophy (abdominal wall protrusion) of the float, hypospadias, and imperforate anus.62,103 Findings such every bit these propose that a thorough search for other built defects is important when examining patients with umbilical hernias.
Omphaloceles are big midline umbilical and skin defects that permit abdominal organs to protrude from the body. Herniated contents are initially covered by a transparent membrane (amniotic tissue) attached to the edges of the umbilical defect until minor trauma ruptures the membrane, exposing the prolapsed contents to contamination (Effigy 84-iv).25,56,62 The incidence of these defects is difficult to determine considering most affected animals either dice or are destroyed without veterinary attention. Attempted surgical repair in i litter of 5-day-old kittens was unsuccessful because tension sutures pulled through the thin abdominal wall.56 Gastroschisis grossly appears like an omphalocele, just the defect is paramedian. This anomaly has been reported in cats and often results in early neonatal death.25
Caused causes of umbilical hernia are uncommon. Umbilical hernias may form from excessive traction on the umbilical cord at parturition. Severance or ligation of the umbilical string too close to the abdominal wall may too create such a defect. Occult congenital umbilical hernias may all of a sudden go clinically evident in adult animals considering of increased intraabdominal pressure from obesity or trauma or with protracted straining.
Umbilical hernias are the most common abdominal hernias in small animals. In an epidemiologic study involving congenital abnormalities found in pet shop dogs over a 2-yr menses, umbilical hernias were found in 0.half dozen% (ten of 1679) of animals.102 Airedale terriers, basenjis, Pekingese, pointers, and Weimaraners are at greater risk.51 The incidence of umbilical hernia is near the aforementioned in cats and dogs when the aforementioned dog breeds at adventure are excluded.99 A loftier incidence of umbilical hernia was noted in one family of Cornish rex cats.99 At that place is no sex predilection for umbilical hernia in the general population; however, females of predisposed dog breeds have a greater incidence of umbilical hernia for unknown reasons.51,99
Diagnosis: Owners usually identify animals with obvious, large umbilical hernias soon after nascency. A patient'due south history and location of the lesion commonly leave little dubiety nearly the diagnosis, although smaller hernias require careful inspection and palpation. Examination of the animal in dorsal recumbency facilitates reduction of the contents of the hernia and hernial ring palpation. Be aware that other masses located in the region of the umbilicus in the puppy or kitten may appear like an umbilical hernia.22
Once an umbilical hernia is found, a conscientious search for other related congenital defects is undertaken. Abdominal radiography is generally not indicated for patients with small, uncomplicated, reducible umbilical hernias. Animals with large umbilical or supraumbilical intestinal wall defects, especially when incomplete caudal sternal fusion is present, are specifically examined for other built diaphragmatic or cardiac defects earlier correction. Animals with multiple built defects, incarcerated hernias, or signs suggesting possible strangulation or obstruction are further examined by radiography, ultrasonography, or both. Dilated, displaced organs exterior the abdominal wall; an obstructive abdominal pattern; or complimentary abdominal fluid may bespeak strangulation. Early surgical exploration should be considered in these patients. Fine needle aspiration of an incarcerated umbilical mass is rarely indicated because cytologic findings are unlikely to change surgical determination making.
Handling: Most small, reducible umbilical hernias in dogs and cats incorporate merely falciform fat and are of little clinical significance. Initially, good for you puppies with small (<2 to 3 mm) hernias are treated conservatively considering spontaneous closure has been reported as late equally 6 months of historic period.97 Afflicted animals are neutered because of genetic predisposition to this affliction.
The decision to repair or to conservatively treat an umbilical hernia depends on the run a risk of potential complications. Hernias with inelastic rings that approximate the size of intestine (i finger size in a pocket-sized to medium-size dog) may be at greater risk for strangulation; the author recommends surgical correction in this instance. Smaller defects or those that are much larger generally do not represent meaning risk to an animal and are dealt with during other constituent surgical procedures or treated conservatively and observed carefully. If surgery is elected in an animal with omphalocele, it is attempted immediately subsequently nascence to help forestall further organ damage or contagion.
When umbilical hernias are corrected at ovariohysterectomy, the hernia repair is completed during routine abdominal wall closure. The initial pare incision is extended cranially over the hernial sac. Alternatively, an elliptical incision is made effectually the base of a large sac to remove redundant tissue. Skin margins are retracted, and the sac is dissected gratuitous. If fat lonely is present in the sac, the neck of the hernia is ligated, and the sac and remaining contents are excised. Small sacs with no internal adhesions can be inverted into the abdomen. Usually, no debridement of wound edges or rectus sheath is required, and closure is routine. Recurrence after repair is uncommon.
Umbilical hernias containing intestinal organs may require more than extensive surgery. The skin incision is made around the base of the hernia, leaving enough skin to close the defect without tension. In incarcerated hernias without strangulation, the hernial sac is dissected complimentary without damaging the contents. The hernial ring is enlarged along the linea alba to release the contents into the belly. The released contents are inspected for viability. Whatever adhesions to the hernial sac or ring are meticulously broken downward. Irreversibly damaged organs or tissues are resected or repaired. The sac is excised, and the hernial ring is debrided if adhesions or scar tissue obscure the edges of the linea alba during closure.
About umbilical hernias can be primarily closed with tension-relieving suture patterns. If the edges of the hernia cannot be apposed easily with thumb forceps, reliance on sutures alone to relieve wound tension is non recommended. Use of a Mayo mattress ("belong over pants") suture pattern for herniorrhaphy is controversial.37,80,109 This pattern permits more contact with apposing wound edges but, in doing so, increases unwanted tension on the repair. Primary side-to-side repairs in humans are superior if wound edges tin can exist apposed without tension.37
In rare situations, absence of a region of the abdominal wall accompanies large umbilical hernias. Releasing incisions tin be made to reduce tension on the main suture line, provided that the rectus muscles and underlying fascia accept adequate force (Figure 84-6). Incisions are fabricated at least 2 cm away from the defect through the external rectus fascia only. The fascia is elevated or dissected off the rectus abdominis muscle and shifted toward the midline, thereby reducing tension on the primary repair. Alternately, a component separation technique can exist utilized to allow a tension-costless midline closure.95 The author prefers to employ prosthetic materials for reconstruction of very big, clean defects rather than rely on shifting local tissues such as fascia (meet Reconstruction of Large Intestinal Hernias later in this chapter).
Animals with supraumbilical hernias and diaphragmatic defects more often than not have enough tissue for routine chief closure. The diaphragmatic hernia is repaired with primary closure showtime so that normal pulmonary function is resumed. Incomplete sternal bones and midline defects are apposed with interrupted sutures of heavy-guess monofilament nylon or polypropylene.
Caudal Abdominal Hernias
Inguinal Hernias
Inguinal hernias are less mutual than umbilical hernias. They result from a defect in the inguinal ring through which abdominal contents protrude.85,125 Inguinal hernia by and large denotes direct and indirect hernias in females and direct hernias in males. Indirect hernias in males are considered separately as scrotal hernias.
Congenital inguinal hernias in dogs and cats are rare and often coexist with umbilical hemias.nine,51,93 Basenji, Pekingese, poodle, basset hound, Cairn terrier, Cavalier King Charles spaniel, Chihuahua, cocker spaniel, dachshund, Pomeranian, Maltese, and West Highland white terrier breeds are predisposed.9,51 Built inguinal hernias develop more often in male dogs than in females, maybe considering of delayed inguinal band narrowing from late testicular descent.38,54,120
Caused inguinal hernias are relatively common in dogs and about often involve eye-aged, intact bitches.83,85,98,120 No breed predilection has been documented,125 although toy-brood dogs and Shar-Peis may be overrepresented. In one case series, female dogs with inguinal herniation were older and significantly lighter than afflicted male dogs. These female dogs belonged to breeds that were overrepresented compared with the general hospital population.9 Sporadic cases of caused inguinal hernias in cats have been described, with equal occurrence in the sexes and breeds examined.51
Anatomy and Pathogenesis: The vaginal process, which contains the spermatic cord in males or the round ligament in females, passes through openings in the caudoventral abdominal wall known as inguinal rings (Figure 84-8). In both sexes, the genital branch of the genitofemoral nerve, artery, and vein and the external pudendal vessels pass through the caudomedial aspect of the canal. The sagittal slit between the abdominal muscles that connects the external and internal inguinal rings is termed the inguinal canal. The internal inguinal ring is bounded medially by the rectus abdominis musculus, cranially by the caudal edge of the internal abdominal oblique musculus, and laterally and caudally past the inguinal ligament. The external inguinal ring is a longitudinal slit in the aponeurosis of the external abdominal oblique muscle. Shut superimposition of the external and internal inguinal rings in minor animals does non grade a truthful "canal," as its name implies, but a potential gap through which hernial disruption may occur. An "interstitial hernia" forms when a construction passes through the internal ring alone without standing past outer wall layers. This condition is described in humans but has not been reported in small animals considering of differences in anatomy of the inguinal culvert (see Figure 84-8).
The pathogenesis of inguinal hernias is uncertain. Few studies have proven a significant heritable influence, except in golden retrievers, cocker spaniels, and dachshunds.66 Inheritance in the last two breeds may exist polygenic.98 Affected small animals should be neutered until evidence excluding heritability every bit a cause of this disease process is conclusive.38
Factors potentially involved in inguinal hernia formation tin be grouped into three major areas: anatomic, hormonal, and metabolic. Enlargement of the archway to the vaginal procedure, which, unlike that in humans, remains open up, is the most of import cause of inguinal hernias in domestic animals.51,125 In humans, a congenital persistent vaginal orifice is essential for evolution of indirect inguinal hernias.6,94 The internal intestinal oblique muscle in humans acts as a shutter to help forestall herniation of abdominal contents with intestinal wrinkle.125 Prevention of inguinal hernias in pocket-size animals may depend on a similar neuromuscular reflex in addition to a normal anatomic barrier at the inguinal rings.72 Bitches may be predisposed because the inguinal canal is shorter and of larger diameter than in males.33 Congenital inguinal hernias may disappear spontaneously at 12 weeks of age because of a subtract in the relative size of the inguinal rings.38 Traumatic inguinal hernias in dogs may result from a preexisting anatomic weakness in the surface area.83
Evidence indicates that sexual activity hormones play an of import role in the crusade of inguinal hernias. In females, most inguinal hernias appear during estrus or in pregnant bitches. Acquired inguinal hernias are much less frequent in neutered females.120 Therefore, estrogen production is considered to have a close relationship to the development of inguinal hernia.98 Sex hormones may modify the strength and grapheme of the connective tissue, weakening or enlarging the inguinal rings.88 Experimentally, a sex hormone imbalance has been direct linked to formation of inguinal hernia in male and female mice.53
A multiinstitutional investigation was undertaken to examine the association between inguinal and perineal hernias in male dogs.104 Amongst male dogs older than 4 years with caused, nontraumatic inguinal hernias, four of the ix dogs described in the literature and all v dogs at one institution had concurrent unilateral or bilateral perineal hernias. Most dogs did not testify marked clinical problems from the perineal hernias, nor were hernias apparent to the owners. In two other studies, three of 11 and ii of 16 males with nontraumatic inguinal hernias had concurrent perineal hemias.9,120 These observations may suggest a like crusade of these concurrent hernias.
Weakening of the abdominal wall may issue from altered nutritional or metabolic condition.85 Obesity increases intraabdominal pressure, forcing intestinal fat through the inguinal canals.83 Furthermore, accumulation of fat effectually the round ligament may dilate the vaginal process and inguinal culvert, allowing hemiation.6
Signalment and Clinical Signs: In general, inguinal hernias are more common in female dogs. In two case series, males accounted for only 8% to 11% of dogs with inguinal hernias.84,113 Of dogs with nontraumatic inguinal hernias, 37% were male.120 Males with inguinal hernias were younger than females and deemed for 5 of viii dogs younger than 2 years.120
Affected animals usually nowadays with a painless, unilateral or bilateral mass with a soft, doughy consistency.9,35,58,83,112 In dogs, more than unilateral inguinal hernias occur on the left side than on the correct.ix,29,120 The external appearance may vary, depending on the amount of vascular occlusion and the nature of the contents. Inguinal hernias may exist undetectably modest. Large hernias may contain a gravid uterus (hysterocele), bladder, or jejunum (Figure 84-9). Large inguinal hernias in bitches that extend caudally following the circular ligament to the vulva may resemble a pendulous perineal hemia.38,83 Direct inguinal hernias in male dogs may be confused with scrotal hernias because of venous or lymphatic obstruction at the inguinal band and subsequent swelling and edema of the testicle and spermatic cord.
Diagnosis: Diagnosis is usually based on celebrated findings and physical exam. Vomiting, abdominal pain, and depression suggest obstructed intestine. In 1 report of dogs with inguinal hernias, airsickness for 2 to 6 days predicted a strangulated small-scale intestine. In that study, all dogs with entrapped, nonviable small intestines vomited, but none of the dogs with inguinal hernias containing viable small intestine vomited.120 History of an inguinal mass and previous vaginal bleeding or belch may indicate uterine involvement. History is usually not helpful for diagnosis of hernias when omentum or fat alone protrudes through the inguinal canals. The risk of strangulated intestine in dogs with long-standing inguinal hernia is less than 5%.120
Diagnosis is confirmed by manual reduction of hernia contents and palpation of the hernial band. Hernia reduction tin be facilitated past elevating the hindquarters with the animate being in dorsal recumbency to reduce caudal intraabdominal pressure. Careful palpation of both inguinal canals is recommended because inguinal hernias can exist bilateral, and small hernias may remain undetected until complications arise.
Incarcerated hernias present more of a diagnostic challenge considering palpation may not yield a diagnosis. All inguinal masses, including mammary tumors and cysts, lipomas, enlarged lymph nodes, abscesses, and hematomas, must be considered every bit differential diagnoses. Although immediate surgical exploration facilitates diagnosis of an inguinal mass or hernia, surgical correction of such disorders should go along with greater precision if the anatomic aspects are delineated outset. The nature of herniated contents can be confirmed with plain or contrast radiography or computed tomography (CT). During image evaluation, particular attention is paid to the caudal abdominal wall structure ("abdominal strip") and the fascial item of the flank musculature; loss of definition in these areas suggests herniation.7 Contents of inguinal hernias may include omentum, fat, ovary, uterus, minor intestine, colon, bladder, or spleen.4,7,9 A herniated gravid uterus is hands detected on plain radiographs by the appearance of the fetal skeleton after 43 days of gestation or, before skeletal ossification, equally a lobulated fluid density.7 The bladder can be identified by taking manifestly radiographs before and after emptying the float by catheterization or with positive or negative dissimilarity cystography. In children with inguinal hernias, pneumoperitoneography has been used to find occult hernias on the contralateral side.48 Fine needle aspiration may help differentiate an inguinal mass from an incarcerated hernia but is rarely used because accidental puncture of a loop of intestine or pyometra could cause leakage and gross contamination.
Surgical Repair: Inguinal hernias are more often than not best repaired at the time of diagnosis; filibuster may result in more difficulty in performing the performance and may increment the risk of complications. Successful surgical repair of inguinal hernias depends on cognition of regional anatomy and advisable surgical technique, which includes apposition of strong tissues without tension and high hernial sac ligation. Simple unilateral inguinal hernias are approached over the inguinal rings. In more complicated hernias (incarcerated or strangulated contents, concurrent serious intraabdominal trauma), the arroyo is first through the ventral midline for exploration; hernia repair is later performed extraabdominally.
Some surgeons repair inguinal hernia through the intestinal crenel.9 With this arroyo, sutures are placed through the parietal peritoneum, the aponeurosis of the transversalis muscle, and the rectus abdominis and internal intestinal oblique muscles.nine Laparoscopic repair of inguinal hernia in afflicted beagle dogs by direct sac ligation or prosthesis onlay has been described in an endosurgery text.116
The conventional surgical approach to inguinal hernias begins with an incision over the lateral aspect of the swelling parallel to the flank fold.58,61,83,112 The hernial sac is exposed through blunt dissection, and the sac and contents are milked or grasped and twisted to gently push the contents through the canal. If the hernia is not easily reducible, the sac is opened (Effigy 84-10), and the canal is enlarged by incising through the inguinal ring in a craniomedial direction. The neck of the hernial sac is ligated as close to the internal inguinal band as possible, and the sac is amputated. The enlarged external inguinal ring and any incisions in the intestinal wall are closed with prolonged absorbable or nonabsorbable sutures. In traumatic inguinal hernias or when the external inguinal band is weak, sutures can be placed between the inguinal ligament, external rectus fascia, and internal oblique intestinal muscle to aid in hernia closure.
A midline arroyo may be preferred over the conventional approach for several reasons (Figure 84-eleven).83,89,124,125 This approach avoids incising through mammary tissue, an advantage especially in a lactating creature. Information technology likewise permits exploration of both inguinal rings, which is recommended past the author because small hernias are frequently missed on palpation.83,89,125 In some animals, mammary tissue must be dissected directly off the external rectus fascia bilaterally to adequately expose the inguinal regions through a midline approach. A single midline incision permits simultaneous hernia repair of uncomplicated bilateral hernias and admission to the abdominal crenel for complicated hernias. Additionally, it is necessary for ovariohysterectomy, which is the simplest option for treatment of a herniated gravid uterus. Successful main repair of the hernia and replacement of the incarcerated uterus can be performed upwards to the seventh week of gestation if a valuable litter is expected. After seven weeks, an ovariohysterectomy or hysterotomy may be recommended before primary hernia repair, depending on the health of the bitch and its value.98
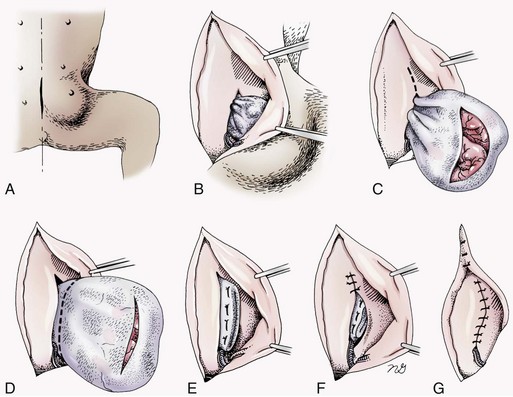
Figure 84-11 Midline approach to inguinal hernia repair. A, Proposed skin incision. B, Approaching the hernial sac by dissecting along the external lamina of the rectus sheath. C, The hernia sac is isolated and opened to expose the contents. The broken line indicates the management of the abdominal wall incision if canal enlargement will facilitate reduction and resection of the hernia contents. D, Hernia contents are reduced and the sac is severed at its base (broken line). E, Hernial sac ligation with horizontal mattress sutures. F, Reduction in the size of the hernial ring with unproblematic interrupted sutures. Yard, Wound closure. Subcutaneous tissue is tacked downwards to the external rectus sheath. (Modified from Smeak DD: Intestinal hernias. In Slatter DH, editor: Textbook of small beast surgery, ed 3, Philadelphia, 2003, Saunders/Elsevier.)
In most animals, inguinal hernias tin be repaired with the patient's own tissues. Patients with large traumatic defects or recurrent inguinal hernias may require reinforcement of the chief hernia repair with prosthetic materials. Inguinal hernias in three intact, small female dogs were successfully repaired past an onlay polyethylene mesh technique.20 A cranial sartorius muscle flap (see Reconstruction of Large Intestinal Hernia department) has been suggested for reconstruction of large inguinal hernias when primary repair is non possible.121 A sartorius musculus flap was used in conjunction with synthetic implants to repair large chronic caudal abdominal hernias in 2 young cats.114
Complications, Aftercare, and Prognosis: The most common complexity later on inguinal hernia repair is hematoma or seroma formation from inadequate hemostasis, extensive tissue dissection during herniorrhaphy, or excessive activity afterwards surgery. Patients are ofttimes reluctant to walk for several days later on surgery, presumably because stretching and motion on the repair cause inflammation and hurting. Swelling and tenderness in the inguinal expanse may also be associated with incorporation of fretfulness and vessels in the hernia repair or ensuing infection. If suppuration occurs, the skin and subcutaneous layers are opened, and local treatment measures are undertaken. Early recognition and treatment of infection reduce the run a risk of hernia dehiscence.109
In a large series of inguinal hernia repairs in dogs, the overall prevalence of postoperative complications was 17%, and the mortality charge per unit was three%. Incisional infection, peritonitis and sepsis, and hernia recurrence were responsible for most postoperative complications. Ane dog died of intestinal dehiscence subsequently resection of an entrapped, nonviable abdominal segment within the hernia.120
Perioperative antibiotics and postoperative bandages are generally not necessary in elementary hernias. If excessive dead space is anticipated, especially subsequently trauma, dressings with or without placement of a closed bleed may assist prevent seroma germination. Exercise is strictly limited until suture removal. Controlled leash walking presently after surgery is encouraged to subtract postoperative edema. The incision is monitored for swelling or belch, and pare sutures are removed in ten to 14 days. Prognosis for uncomplicated repair of inguinal hernia is expert to fantabulous. In one study, all just one of 61 dogs with inguinal hernias survived.9
Scrotal Hernia
Anatomy and Pathogenesis
Scrotal hernias are indirect hernias that consequence from a defect in the vaginal band, allowing abdominal contents to protrude into the vaginal procedure aslope spermatic string contents (see Effigy 84-7).78 Herniated organs within the vaginal procedure practice not necessarily have to extend as far distally as the scrotum for the condition to exist considered a scrotal hernia. These hernias are rare, peculiarly in cats.35,67,76 Most instance reports involve young male dogs.* Dog breeds with scrotal hernias are generally larger than breeds of female dogs with inguinal hemias.nine Strangulation of contents occurs more frequently in male dogs with scrotal hernias than in females with indirect inguinal hernias.98,120 In a study of 35 dogs with inguinal hernias, five had strangulated bowel, and four were young male dogs.120
Literature regarding the pathogenesis of scrotal hernias is limited. Dissimilar the situation in humans, heritability of this disorder in dogs and cats remains unknown. A congenital anatomic defect or weakness may exist present in the vaginal orifice in dogs with scrotal hemias.125 Occasionally, scrotal hernia formation is associated with trauma.25 Ectopic testes accept been reported in 19% to 33% of male dogs with inguinal hemias.113,120 An increased risk for inguinal hernias was establish in dogs with cryptorchidism.90
The anatomic boundaries of the inguinal rings are described earlier (see Inguinal Hernia section). The relative size of the inguinal canal and the structures found within the inguinal rings differ between the sexes. The cremaster muscle in males is a continuation of the costless caudal border of the internal oblique intestinal musculus. Normal contents of the spermatic cord (ductus deferens and associated artery and vein and testicular avenue, vein, and nerves) pass through the inguinal rings within the vaginal process.
Clinical Signs
Presenting signs of scrotal herniation result from protrusion of intestinal contents through the vaginal process, causing hurting, swelling, and oftentimes organ dysfunction. Scrotal hernia is predominantly unilateral, with equal occurrence on both sides, although several bilateral cases take been reported.nine,25,33,47 In humans, 15% of patients with unilateral scrotal hernia eventually developed a contralateral hernia; therefore, it would seem prudent to consider inspecting the contralateral inguinal band in animals with unilateral scrotal hernia.96
The reported contents of scrotal hernias include periprostatic fat, omentum, and intestine.47,58 The external appearance of scrotal hernia depends on the sac contents and amount of vascular obstruction at the hernial band. Swelling is generally cordlike, extending from the inguinal band to the caudal aspect of the scrotum (Figure 84-12).67 Strangulated hernias have a nighttime discoloration of the tissues within the hernia, which is ofttimes visible externally. Signs of abrupt pain are commonly exhibited during palpation of the hernia.
< div grade='tao-gold-member'>

Source: https://veteriankey.com/abdominal-wall-reconstruction-and-hernias/
Posted by: houstonbeturped.blogspot.com
0 Response to "Can A Strangulated Hernia Repair Itself"
Post a Comment